The note is done before you leave the room.
One platform for independent primary care — EHR, scheduling, and revenue cycle in one login.
FHIR-native · TEFCA-connected · Structure-first ambient scribe · Turn-key RCM
The state of independent primary care
Your EHR takes your evenings and leaks your revenue.
Squeezed from both sides — documentation burden grows, billing tools let earned revenue slip away.
Two promises
Everything in the platform serves one of two outcomes.
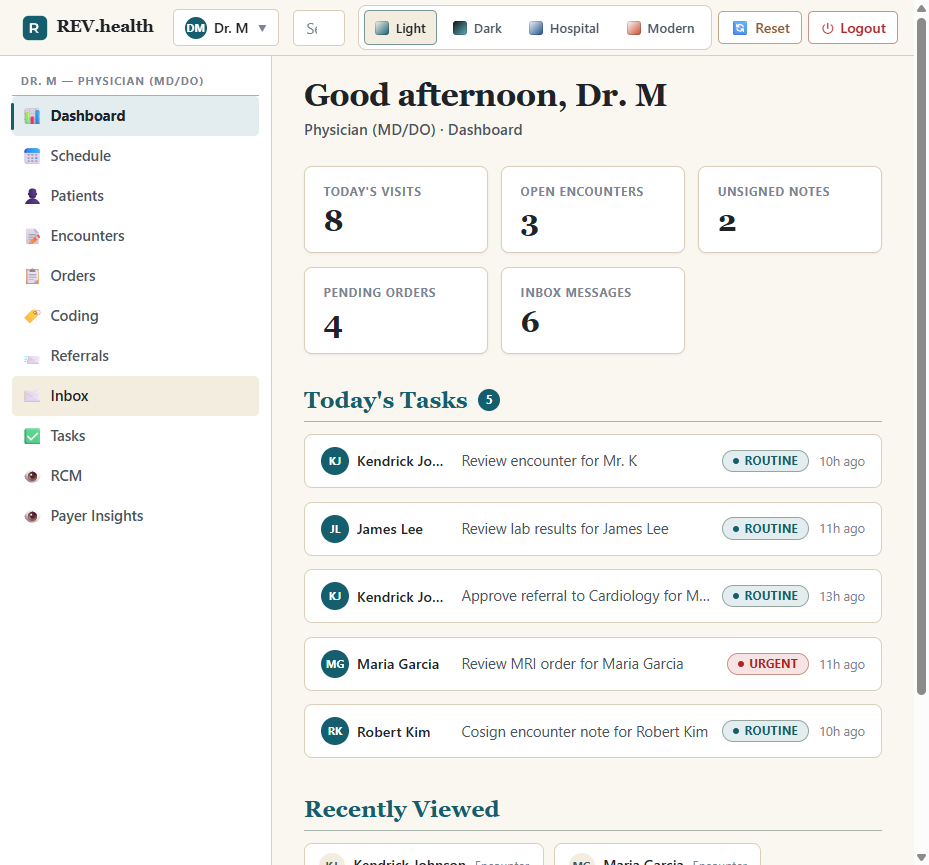
The note is done before you leave the room
Talk to your patient. The scribe fills coded fields — median charting after the visit: under 90 seconds.
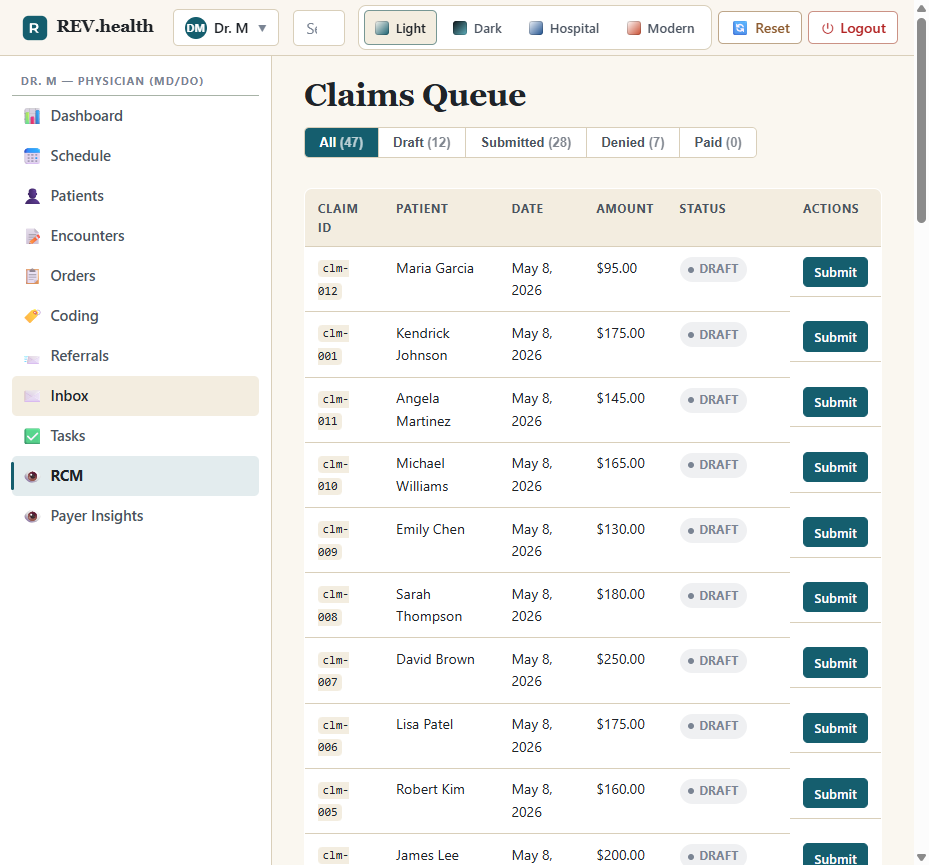
Paid correctly the first time
Eligibility, coding, scrubbing, posting, appeals — one pipeline. Target: ≥98% first-pass clean.
One visit, end to end
A day that runs on time.
Patient self-schedules at 9 pm
Resource-feasible openings, eligibility checked, cost estimate at booking.
Coverage verified before arrival
270/271 at booking, T-24h, and check-in — not as a denial weeks later.
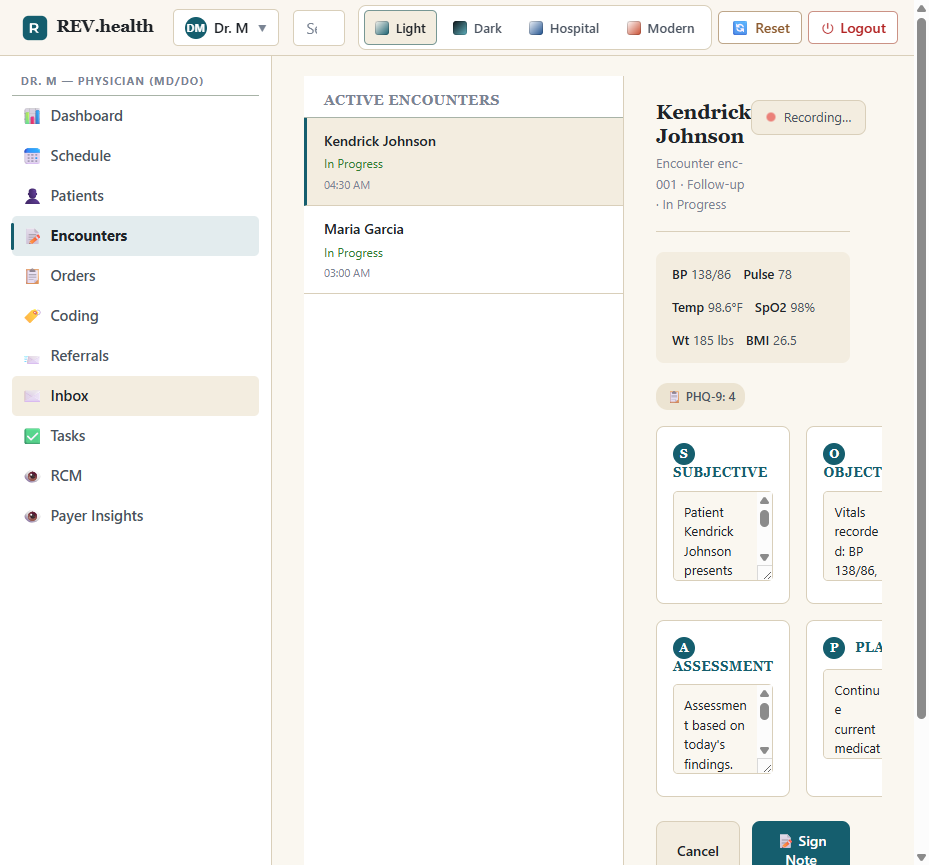
The clinician talks; the form fills
A structured draft note within 60 seconds of “End encounter.”
Sign once — the claim builds itself
Charges captured, claim scrubbed, 837P out the same day.
The platform
Ten modules. One record. Zero bolt-ons.
One platform replaces the EHR, the PM suite, the clearinghouse glue, and the back-office RCM tooling.
Clinical Documentation
Structure-first ambient scribe.
Note signed before you leave →Scheduling
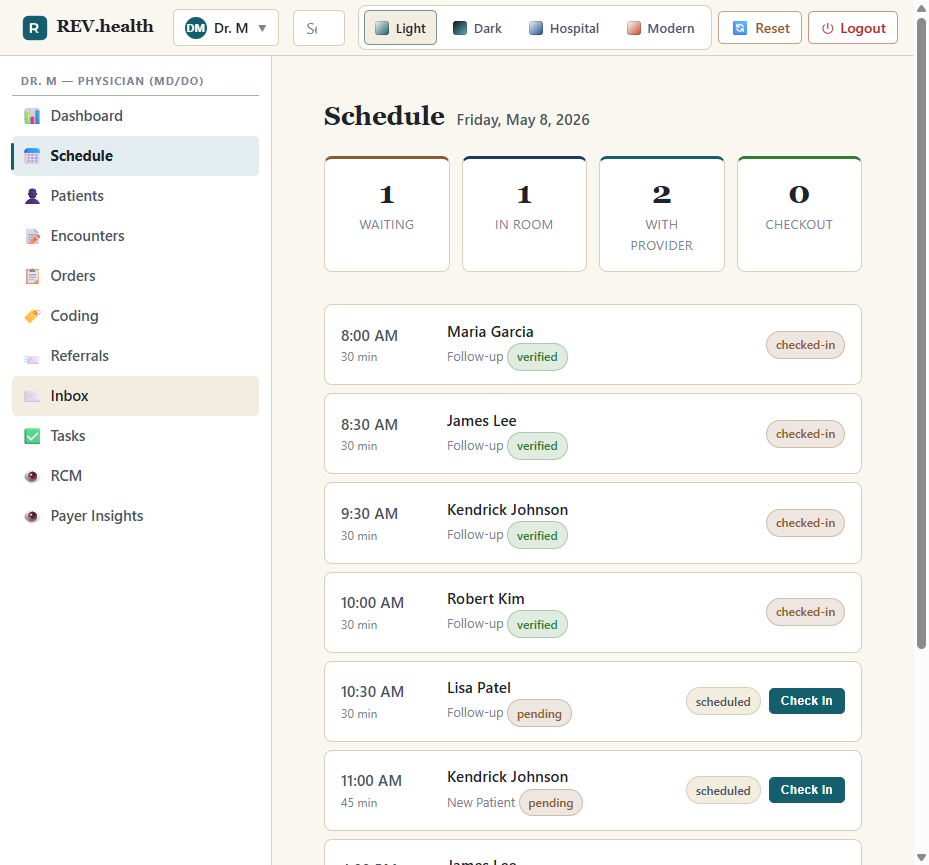
Resource-graph, minute-level.
95th-percentile wait ≤12 min →Eligibility & Prior Auth
Real-time benefits, electronic PA.
Coverage facts before the visit →Coding & CDS
Evidence-linked codes, CDS Hooks 2.0.
Code while you document →eRx & EPCS
Surescripts, RTPB, PDMP, two-factor.
One screen replaces phone + fax →Referrals
Closed-loop, bidirectional.
Send with full records in <60s →Revenue Cycle
Scrub → 837P → 835 → appeal. Turn-key.
≥98% first-pass clean →Patient Portal
Patients are users, your brand.
Your brand, their record →Task Management
FHIR Task work queues, SLAs.
Nothing falls through →Payer Optimization
Compliant, opt-in analytics.
Compliant by construction →One record underneath it all
Clinical data belongs to the patient. Operational data stays per-practice. Every read is audited.
Why rev.health is different
Built for the 2026–2027 regulatory window.
FHIR-native, AI-native, and TEFCA-connected from day one — not retrofitted.
Structure-first ambient scribe
Bounded, coded fields — not free-text guesswork.
Resource-graph scheduling
A constraint solver re-optimizes the day in real time.
Turn-key RCM, no hidden hires
Charge capture through appeals, run by the platform.
Patients are users
The same signed note, carried across practices.
FHIR-native, TEFCA-connected
US Core FHIR is the native surface, not an export.
Every read is auditable
Read-access audit on every chart view, shown to the patient.
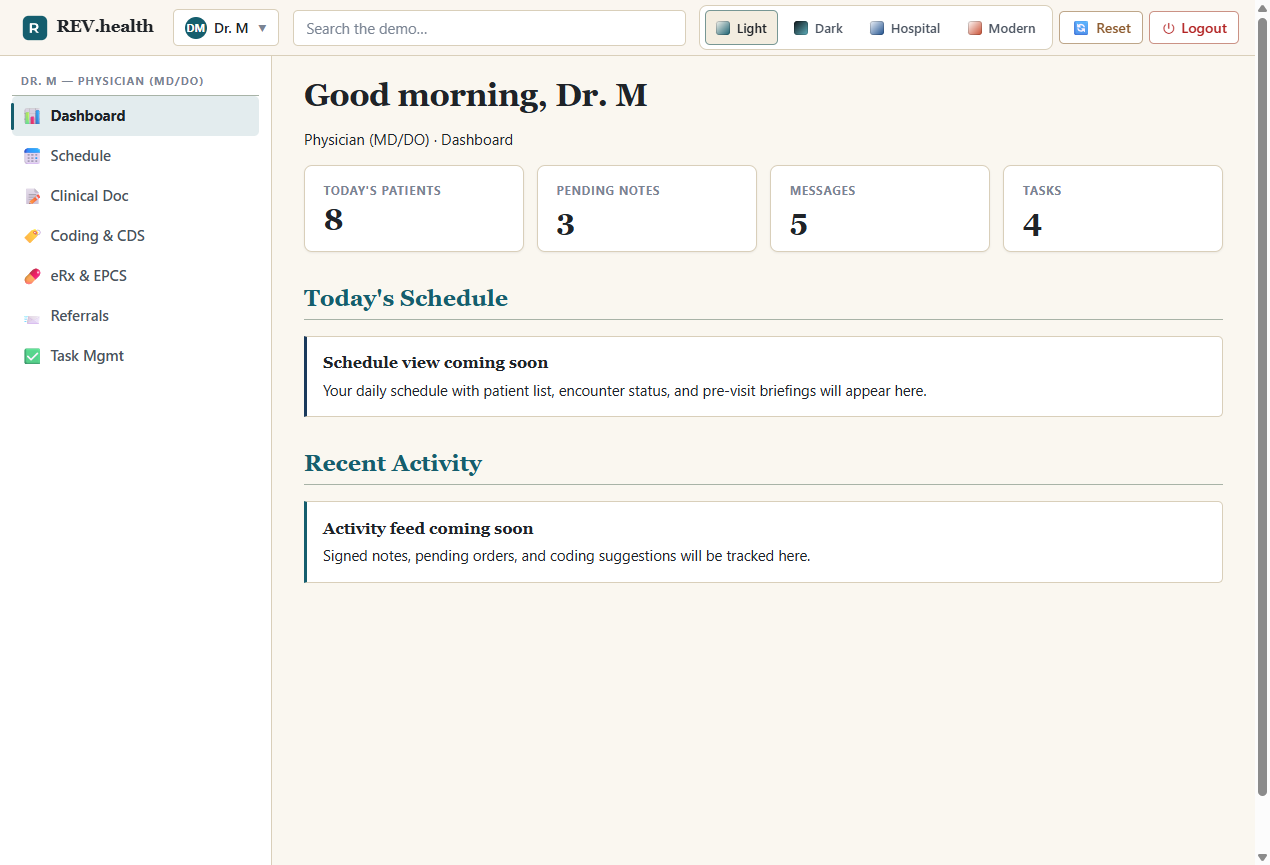
Designed to be lived in
One platform. Every workflow. All day long.
The same practice, from the morning schedule to the signed note to the clean claim.
Why practices switch
The incumbents have outgrown you — or never grew up.
Cloud suites price like enterprise software and staff their gaps with your hires. Small-practice tools never built billing.
| Vendor | Pricing reality | The catch |
|---|---|---|
| athenahealth | 4–7% of collections + ~$140/provider/mo | RCM not turn-key; needs a billing-coordinator hire. |
| eClinicalWorks | $449–599/provider/mo + 2.9% RCM | $155M DOJ settlement over certification & audit logs. |
| NextGen | $150–500/provider/mo; quote-based | 2023 breach hit ~1.05M; $19.375M class action. |
| Elation | Loved EHR, billing sold separately | No integrated RCM — a second vendor contract. |
| rev.health | $399/MD-DO · $299/PA-NP + 3.5% RCM. Published. | EMR + PM + turn-key RCM, everything included. |
Security & compliance
Compliance is the product floor, not the marketing ceiling.
Engineered against the full 2026–2027 regulatory stack — with an honest line between certified, in progress, and roadmap.
Pricing
One price. On the website. Like software should be.
No quote theater, no percentage that “varies,” no surprise hires to make the billing work.
Everything is included — scribe, scheduling, eligibility, coding, eRx, referrals, portal, tasks. RCM is the only usage-based line.
- Ambient scribe included — not a $125/mo add-on
- Unlimited front-desk, MA, and billing staff seats
- Self-serve data egress — your data leaves when you do
How that compares
At $1M in annual collections for a two-clinician practice, typical incumbent stacks run:
| Stack | Approx. annual cost |
|---|---|
| athenahealth bundled (4–7% of collections) | $40K–70K + a billing-coordinator hire |
| eClinicalWorks + 2.9% RCM | ~$34K + DOJ-settlement vendor risk |
| Lightweight EHR + ambient scribe add-on + outsourced biller | 3 contracts, 3 logins, 3 ways to drop a claim |
| rev.health, all-in | 2 MD/DO: $9.6K SaaS + $35K RCM = ~$44.6K, everything included |
The difference isn't only the sticker. It's the ~1.5 clinician-hours returned per day, the denials that never happen, and the biller you don't have to hire to babysit your billing vendor.
Leadership
Built by people who've lived the problem.
An investor-operator, a product-and-engineering founder, and a practicing physician — aligned on giving independent practices their time and their margin back.
 PF
PF JH
JH DD
DDAdvisory board in formation: an RCM operator, a health-IT regulatory expert, and practicing primary-care physicians.
Design partner program
We're onboarding a small cohort of independent practices.
Design partners get white-glove migration, direct access to the product team, locked-in founding pricing, and a real say in what ships next. We're looking for owner-operated primary care practices of 1–5 clinicians who are done with their current stack.
- Founding-cohort pricing, locked for 3 years
- Dedicated migration engineer — charts, schedules, balances
- Weekly office hours with the product team
- Cancel anytime; your data exports itself