Home / Platform / Clinical Documentation
Module 01 · Structure-first ambient scribeGive the exam room back to the patient.
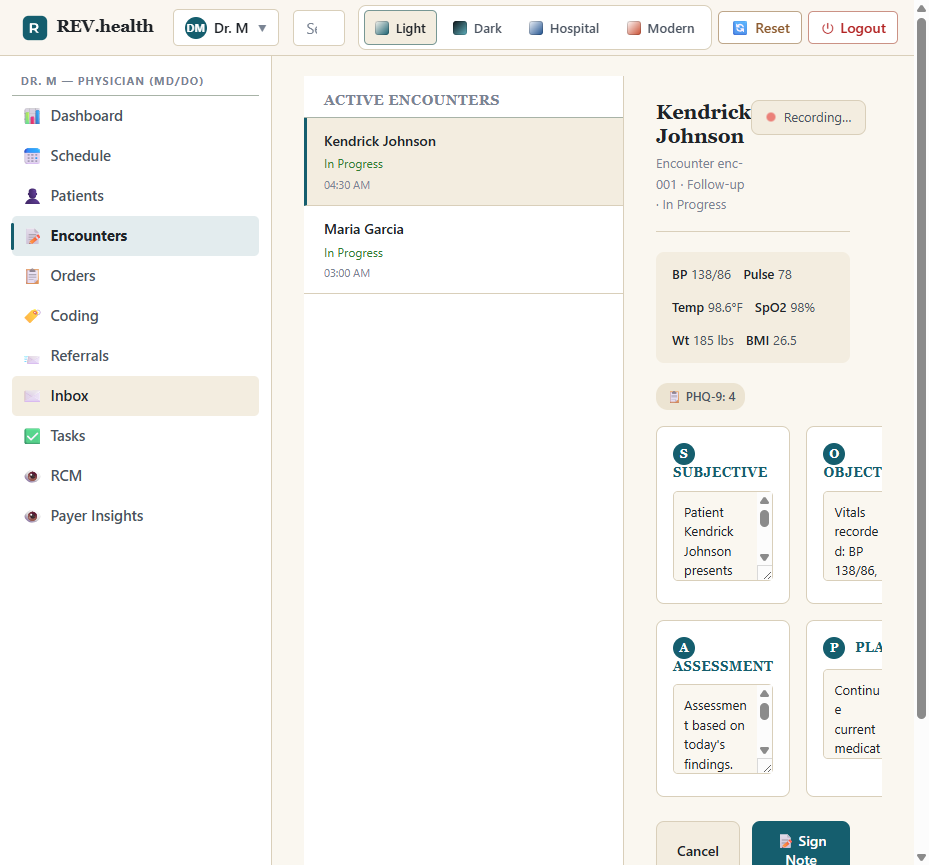
Tap once, stop typing, sign on the way out. The note is structured, coded, and traced to the audio that justifies it.
The signature mechanic
Ambient audio in. Coded, evidence-linked fields out.
The conversation becomes diarized utterances; the model proposes structured clinical facts; each fact keeps a link back to the exact 5-second window of audio that justifies it. Nothing reaches the chart until you accept it.
A bolt-on scribe would stop at the prose. rev.health's ScribeStructuredOutput rows each carry an evidence-utterance range, so click-to-play works from any signed note line back to the audio — and the write-back to the patient's global record is atomic with its source-org stamp.
The problem
Bolt-on scribes generate prose. Your chart needs structure.
Most ambient scribes stop at a draft note. The free text still has to be reconciled into the problem list, the medication list, and the order set by hand — the clinician saves time on typing and spends it on plumbing.
AI is imperfect — so we add structure. Every encounter becomes a versioned form: the clinician talks; the platform fills bounded, coded fields. Each visit teaches the form, and the forms evolve toward steadily more efficient and more accurate encounters.
rev.health rejects the prose-only split. The scribe is not a peripheral — it is a first-class data source whose output writes directly into the chart's structured fields, with the audio transcript and timestamp captured as provenance on every fact.
The scribe proposes structured updates — new problems (SNOMED-CT + ICD-10 coded), medication changes, allergies, orders. You review, accept, and sign. The platform handles everything downstream: the codes, the charges, the claim.
Key capabilities
What ships in the documentation surface.
Pre-visit briefing
A one-screen chart summary before you walk in: last visit, active problems, meds, allergies, due preventive care, recent labs — plus an outside-records snapshot pulled via TEFCA. Built from the patient's global record, not just your practice's slice.
One-tap ambient capture
A single button opens the visit's versioned form and starts capture from the room iPad, in-room mic, or paired phone. Patient consent is captured before recording begins. Real-time transcription with speaker diarization.
Structured draft in 60 seconds
Within a minute of “End encounter,” the draft note is ready: HPI, ROS, PE, A/P. Click any sentence and play the 5-second audio clip that justifies it.
Structured write-back
The defining capability. The scribe proposes coded problem-list entries, medication changes, allergies, and orders. On accept, each becomes a global clinical fact with full source attribution — not free text trapped in a note.
SOAP or APSO — your call
First-class support for traditional S→O→A→P and assessment-first A→P→S→O layouts. Per-clinician toggle, persisted; the underlying data model is identical.
Real-time coding suggestions
As the note takes shape, ICD-10-CM, SNOMED-CT, CPT, and E/M level suggestions appear with MDM rationale — each linked to the audio evidence that supports it. See Coding & CDS →
Review queue & undo
Nothing reaches the global record until you sign. A 24-hour undo window covers write-backs; afterwards, retraction becomes a versioned correction with the original preserved in the audit trail.
Encounter templates
Annual wellness, acute, follow-up, telehealth, Medicare AWV — templates pre-load relevant note sections, screening prompts, and order-set candidates. Curated primary-care defaults ship in the box.
Bilingual capture
Spanish-English visits transcribe in both languages with diarization labeling speaker and language; the structured note generates in English with original-language utterances preserved for evidence review.
The data model
Eight objects turn a conversation into a defensible chart.
The split is deliberate: the act of producing a note (audio, transcript, proposals, review) is the practice's operational data; the clinical fact it produces belongs to the patient and lives in the global record with a source-org stamp.
Encounter & EncounterNote
The visit shell, opened at check-in and closed at “End encounter,” and its versioned SOAP/APSO note. Every correction is a new version — the original never leaves the audit trail.
ScribeSession
One capture session: consent flag and method recorded before a byte of audio is persisted, encrypted at rest, retained 365 days by default (configurable to 10 years), purged automatically while transcripts remain.
ScribeUtterance
The diarized transcript layer — one row per utterance with speaker label, millisecond offsets, BCP-47 language, and ASR confidence. The raw evidence the note is built from.
ScribeStructuredOutput
The bridge to the chart: each proposed fact (problem, med change, allergy, order, note line) references the utterance range that supports it and carries model name + version for DSI transparency.
ScribeReviewState
Per-proposal review — accept, accept-edited, reject, defer, undo. Nothing is promoted to a global fact without an accept; the reviewer and timestamp are recorded.
Problem & ProblemList (global)
The patient's longitudinal list — deliberately not org-partitioned. Each fact carries SourceOrganizationID, SNOMED-CT + ICD-10 codes, and FHIR Condition clinical/verification status.
Functional & non-functional targets
What the implementation is bound to.
The pipeline, in requirements
- Pre-visit briefing assembled from the patient's global Problem, Med, Allergy, Lab, and Imaging records plus TEFCA outside records
- Consent captured before any audio is written to durable storage
- Structured proposals produced within 60 seconds of session end
- Click-to-play from any signed note sentence to its 5-second audio clip
- Nothing promoted to a global fact without an explicit accept
- 24-hour retraction window; afterwards a versioned correction
- Every read of a note, problem, or transcript writes a read-access audit record
The numbers behind them
| NFR | Target |
|---|---|
| End-encounter → draft note latency | ≤ 30s median · ≤ 60s p95 |
| Word error rate (clinical eval set) | ≤ 6% |
| Hallucinated PE findings | ≤ 1% |
| Scribe capture availability | 99.9% monthly |
| Throughput (5 clinicians, 28 visits/day) | ≥ 140 sessions/day, queue p95 < 3 min |
| Offline audio buffering on capture outage | up to 4 hours, no loss |
Workflow
The 18-minute follow-up that ends in the room.
Open the pre-visit briefing
Last week's HbA1c and the home BP log the patient submitted through the portal are already on screen.
Tap “Start scribe,” confirm consent
Then spend the next 16 minutes talking. No laptop. No clipboard. Eye contact.
Tap “End encounter”
By the time you reach the workstation the structured draft is ready — HPI, ROS, PE, A/P, with an evidence link on every line.
Review the proposals
“Type 2 diabetes mellitus without complications” for the problem list, metformin 500 mg PO BID as an order — accept both with two taps.
Sign
The note is signed, the chart is updated, the charge is captured. Total visit: 18 minutes. Pajama time: zero.
Three years later
The audit-defensible note.
A payer audit lands on a level-4 E/M visit. The auditor asks for documentation of medical decision-making complexity. Your compliance officer pulls the signed note — every A/P line carries an evidence-link button. Clicking “discussed risk of progression to diabetic nephropathy” plays a 7-second clip of you explaining exactly that.
The auditor doesn't just see a note. They see the conversation that produced it.
Who benefits
18–28 patients a day, eyes on the patient, note signed before the last patient of the day leaves. Owns clinical accuracy; the platform owns the plumbing.
Rooms the patient with the briefing on the iPad; vitals, med rec, and structured intake are half-done before the clinician walks in — with the MA's own contributions attributed in the audit trail.
Consents to recording at the start of the visit and reads the same signed note in the portal — the actual note, not a redacted summary.
Audits consent capture, audio retention, access logs, and the evidence chain behind every note line — from one surface.
Performance targets
The numbers this module is built to hit.
| Metric | Target |
|---|---|
| Charting time per visit (end-encounter to sign-off) | ≤ 90 seconds median · ≤ 4 minutes p95 |
| After-hours pajama time | ≥ 60% reduction within 90 days of go-live |
| Draft note latency after “End encounter” | ≤ 60 seconds p95 |
| Structured write-back acceptance without edit | ≥ 70% |
| Notes signed before the clinician leaves clinic | ≥ 80% |
| Hallucinated physical-exam findings | ≤ 1% on sampled audit sets |
| Evidence-link coverage on signed A/P sentences | 100% — gaps block sign-off |
Connected modules
Where the signed note goes next.
Coding & CDS
Consumes the structured A/P to propose ICD-10, CPT, and E/M codes with evidence links.
Module 04 →Revenue Cycle
The signed, coded note becomes a scrubbed claim — automatically, the same day.
Module 07 →Patient Portal
Renders the same signed note for the patient, with the same evidence-link affordances.
Module 08 →Zero pajama time is a feature. Ship it to your practice.
Join the design-partner cohort and put the structure-first scribe in your exam rooms.
Join the waitlist